

Last week I posted about RFKJ’s ill-informed and irresponsible effort get doctors to take patients off anti-depressants, especially SSRIs. It seems the discussion has centered on the SSRI withdrawal symptoms. No one, it seems was talking about the risk of causing recurrence of depression and an increase in suicide and homicide. I did a video on this the other day.
Well of course, someone took issue with my argument and demanded proof. So, I did a search using the New England Journal of Medicine tool - “Open Evidence”. I asked, what does the medical literature have to say about the issue of stopping anti-depressants and the risk of recurrent depression with suicidal and homicidal ideation.
https://www.openevidence.com/ask/21187043-f240-41c9-9fe1-5c10ee2fd303
The medical literature provides substantial evidence on antidepressant discontinuation and its relationship to depression relapse, suicidal ideation, and — to a lesser extent — aggressive behavior, though data on homicidal ideation specifically are very limited.
Depression Relapse After Antidepressant Discontinuation
A large meta-analysis of 40 studies (n = 8,890) found that discontinuing antidepressants approximately doubles the risk of depressive relapse compared to maintenance therapy (relapse rate 39.7% vs. 20.9%; OR 0.38 favoring continuation). [1] The landmark ANTLER trial (NEJM, 2021) confirmed this in a primary care population: 56% of patients who discontinued relapsed within 52 weeks, compared to 39% in the maintenance group (HR 2.06; 95% CI, 1.56–2.70). [2] A 2024 meta-analysis found the 6-month relapse rate after discontinuation was approximately 35%, rising to 45% at 12 months, with treatment duration of less than 3 months carrying the highest relapse risk. [3]
Among patients in primary care practices who felt well enough to discontinue antidepressant therapy, those who were assigned to stop their medication had a higher risk of relapse of depression by 52 weeks than those who were assigned to maintain their current therapy.
— Gemma Lewis, Ph.D., et al., University College London and other institutions
Maintenance or Discontinuation of Antidepressants in Primary Care. N Engl J Med. September 29, 2021.
Used under license from The New England Journal of Medicine.
The following table from the ANTLER trial illustrates the primary and secondary outcomes comparing maintenance versus discontinuation groups:
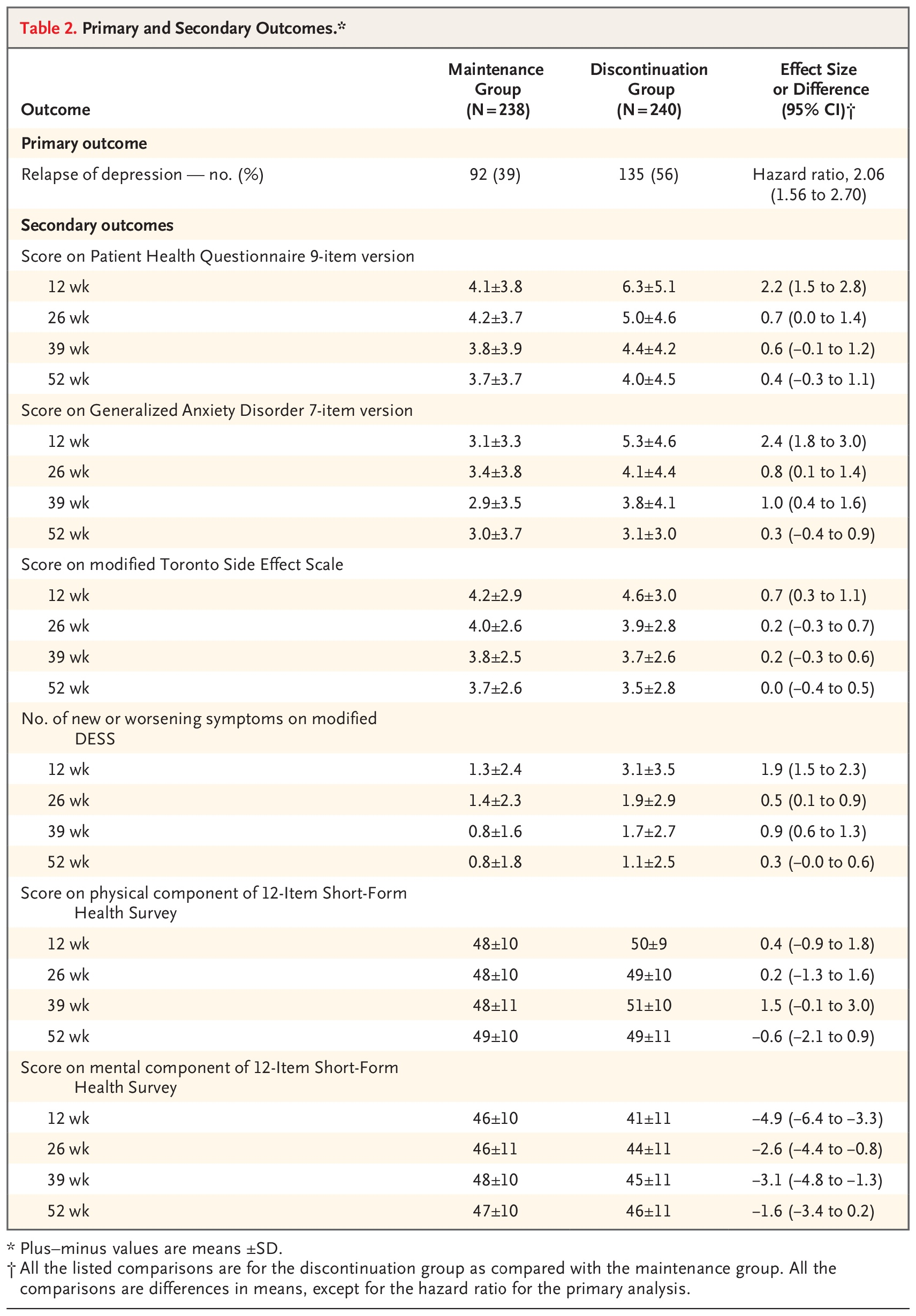
Table 2. Primary and Secondary Outcomes.*
Maintenance or Discontinuation of Antidepressants in Primary Care. N Engl J Med. September 29, 2021.
Used under license from The New England Journal of Medicine.
Current guidelines recommend maintenance therapy for at least 6–9 months after a first episode and at least 2 years for recurrent or severe illness. [4]
Suicidal Ideation and Behavior After Discontinuation
A large nested case-control study (n > 50,000) found that antidepressant discontinuation was associated with a significant increase in suicide attempt risk (OR 1.61, p < 0.05), while ongoing antidepressant use was protective (OR 0.62, p < 0.001). [5] A UK cohort study of nearly 239,000 patients found that rates of attempted suicide or self-harm were increased in the first 28 days after stopping treatment, mirroring the elevated risk seen in the first 28 days after initiation. [6] A Cochrane review identified several trials reporting higher suicidality scores in discontinuation groups, though data were too heterogeneous to pool. [7]
Importantly, the FDA black box warning on antidepressants addresses increased suicidal thoughts and behavior in children, adolescents, and young adults (under age 25) during treatment initiation and dose changes — and guidelines also recommend monitoring after stopping treatment. [8-10] A 2026 Lancet review explicitly recommends routine monitoring of suicide “particularly at the outset following the initiation of a new medication, and also after stopping treatment“. [9]
It should be noted that a 2025 JAMA Psychiatry meta-analysis found that mood worsening in the first 1–2 weeks after discontinuation was not significantly associated with antidepressant cessation itself (suggesting early mood changes may reflect discontinuation syndrome rather than true relapse), but that depression relapse occurring later (beyond the first few weeks) is a genuine clinical concern. [11]
Aggressive and Homicidal Behavior
Evidence specifically linking antidepressant discontinuation to homicidal ideation is extremely limited in the medical literature. However, several related findings are relevant:
A systematic review of clinical study reports from SSRIs and SNRIs found that antidepressant use was associated with increased aggressive behavior overall (OR 1.93; 95% CI, 1.26–2.95), with the effect most pronounced in children and adolescents (OR 2.79; 95% CI, 1.62–4.81). [12]
SSRI discontinuation has been associated with irritability, sudden outbursts of anger, agitation, and impulsive behavior as part of the discontinuation syndrome. These symptoms are recognized in the DSM-5 description of antidepressant discontinuation syndrome. [7][13-14]
A Danish cohort study noted that postmarketing surveillance and case reports have indicated associations between antidepressant medication and increased risk of criminal and aggressive behavior, though this was primarily studied in the context of treatment initiation rather than discontinuation. [15]
No well-powered controlled studies have specifically examined homicidal ideation as an outcome of antidepressant discontinuation.
Clinical Implications
The highest-risk periods for suicidal behavior are treatment initiation, dose changes, and discontinuation. [5-6] When discontinuation is planned, gradual tapering is recommended, though evidence on optimal tapering strategies remains limited — a 2026 network meta-analysis noted that comparative evidence on different tapering rates and adjunctive psychological support is “scarce and inconclusive”. [4] Close monitoring during and after discontinuation is essential, particularly for patients with a history of recurrent depression, prior suicidal behavior, or aggressive tendencies.
1.
Molecular Psychiatry. 2021. Kato M, Hori H, Inoue T, et al.SR
2.
Maintenance or Discontinuation of Antidepressants in Primary Care.

The New England Journal of Medicine. 2021. Lewis G, Marston L, Duffy L, et al.RCT
3.
Psychiatry Research. 2024. Hu Y, Xue H, Ni X, et al.SR
4.

The Lancet. Psychiatry. 2026. Zaccoletti D, Mosconi C, Gastaldon C, et al.NewSR
5.
The Journal of Clinical Psychiatry. 2009. Valuck RJ, Orton HD, Libby AM.
6.

BMJ. 2015. Coupland C, Hill T, Morriss R, et al.
7.

The Cochrane Database of Systematic Reviews. 2021. Van Leeuwen E, van Driel ML, Horowitz MA, et al.SR
8.
Suicide and Suicide Risk in Adolescents.

Pediatrics. 2023. Hua LL, Lee J, Rahmandar MH, Sigel EJ.Guideline
9.
Lancet. 2026. Malhi GS, Bell E, Stavdal A, et al.NewReview
10.
Fluoxetine. FDA Drug Label.

Food and Drug Administration. Updated date: 2025-09-30.
11.
Incidence and Nature of Antidepressant Discontinuation Symptoms.

JAMA Psychiatry. 2025. Kalfas M, Tsapekos D, Butler M, et al.NewSR
12.
BMJ. 2016. Sharma T, Guski LS, Freund N, Gøtzsche PC.SR
13.
Newer Antidepressants and the Discontinuation Syndrome.
The Journal of Clinical Psychiatry. 1997. Haddad P.Review
14.
Diagnostic and Statistical Manual of Mental Disorders.
American Psychiatric Association (2022). 2022. Dilip V. Jeste, Jeffrey A. Lieberman, David Fassler, et alGuideline
15.
Acta Psychiatrica Scandinavica. 2019. Osler M, Wium-Andersen MK, Wium-Andersen IK, et al.
