

This was posted on Doximity today by First10EM.com
It caused me to take a step back. I have been prescribing Paxlovid for years and believed it was very effective. What gives?
So I checked with NEJM Open Evidence. Here is what I got back.
According to the FDA-approved drug label, Paxlovid (nirmatrelvir/ritonavir) is indicated for the treatment of mild-to-moderate COVID-19 in adults at high risk for progression to severe COVID-19. Treatment should be initiated as soon as possible after diagnosis and within 5 days of symptom onset. The recommended dosage is 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir, taken together twice daily for 5 days. In the pivotal EPIC-HR trial, the relative risk reduction for COVID-19-related hospitalization or death through day 28 was 86% (95% CI: 72%, 93%) in the mITT1 population, with an absolute risk reduction of 6.5% (95% CI: 3.7%, 9.3%; p 0.0001). [1]
Pivotal Randomized Controlled Trial (EPIC-HR)
The landmark evidence comes from the EPIC-HR trial, a phase 2–3 double-blind RCT of 2,246 symptomatic, unvaccinated, nonhospitalized adults at high risk for severe COVID-19. Treatment initiated within 3 days of symptom onset resulted in an 89.1% relative risk reduction in COVID-19-related hospitalization or death by day 28 (0.77% vs. 7.01%; absolute difference −6.32 percentage points; P<0.001). This efficacy was maintained in the full modified intention-to-treat population (88.9% relative risk reduction). Notably, all 13 deaths occurred in the placebo group. Nirmatrelvir also significantly reduced viral load at day 5 (adjusted mean difference −0.868 log₁₀ copies/mL). Adverse events were similar between groups, with dysgeusia (5.6% vs. 0.3%) and diarrhea (3.1% vs. 1.6%) more common with treatment. [2]
The following figure from the EPIC-HR trial illustrates the primary efficacy results, including Kaplan-Meier curves and subgroup analyses demonstrating consistent benefit across patient populations.
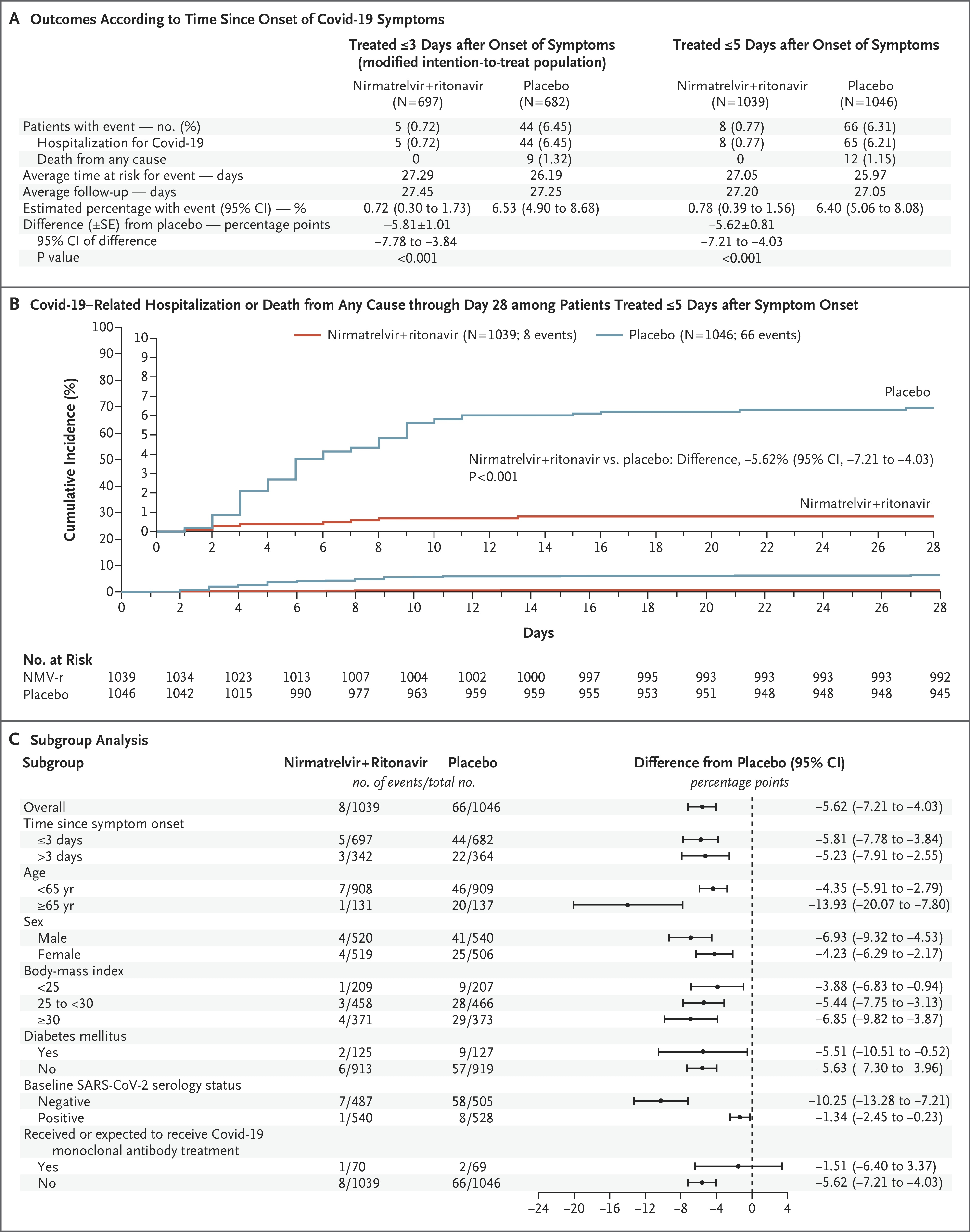
Figure 2. Efficacy of Nirmatrelvir plus Ritonavir (NMV-r) in Preventing Covid-19–Related Hospitalization or Death from Any Cause through Day 28.
Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. N Engl J Med. April 13, 2022.
Used under license from The New England Journal of Medicine.
EPIC-SR Trial (Vaccinated/Standard-Risk Patients)
The EPIC-SR trial enrolled vaccinated or unvaccinated adults at standard or high risk for severe COVID-19. There was no significant difference in time to symptom alleviation between nirmatrelvir-ritonavir and placebo. However, numerically fewer hospitalizations or deaths occurred in the treatment group (5 vs. 10), and among high-risk participants specifically, the difference was −1.3 percentage points (95% CI: −3.3 to 0.7) — not statistically significant but directionally consistent with benefit. [3]
PANORAMIC Trial (Higher-Risk Outpatients, Omicron Era)
The UK-based PANORAMIC trial randomized 3,371 higher-risk outpatients during the Omicron era. Nirmatrelvir-ritonavir did not significantly reduce hospitalization or death (0.8% vs. 0.7%; OR 1.18, 95% BCI 0.55–2.62), likely reflecting the very low baseline event rate in a highly vaccinated population. However, it significantly accelerated symptom recovery: early sustained recovery by day 14 occurred in 33.0% vs. 22.1% (OR 1.74, 95% BCI 1.48–2.04), with median time to recovery of 14 vs. 21 days. Viral load at day 5 was also significantly lower with treatment (geometric mean ratio 0.13). [4]
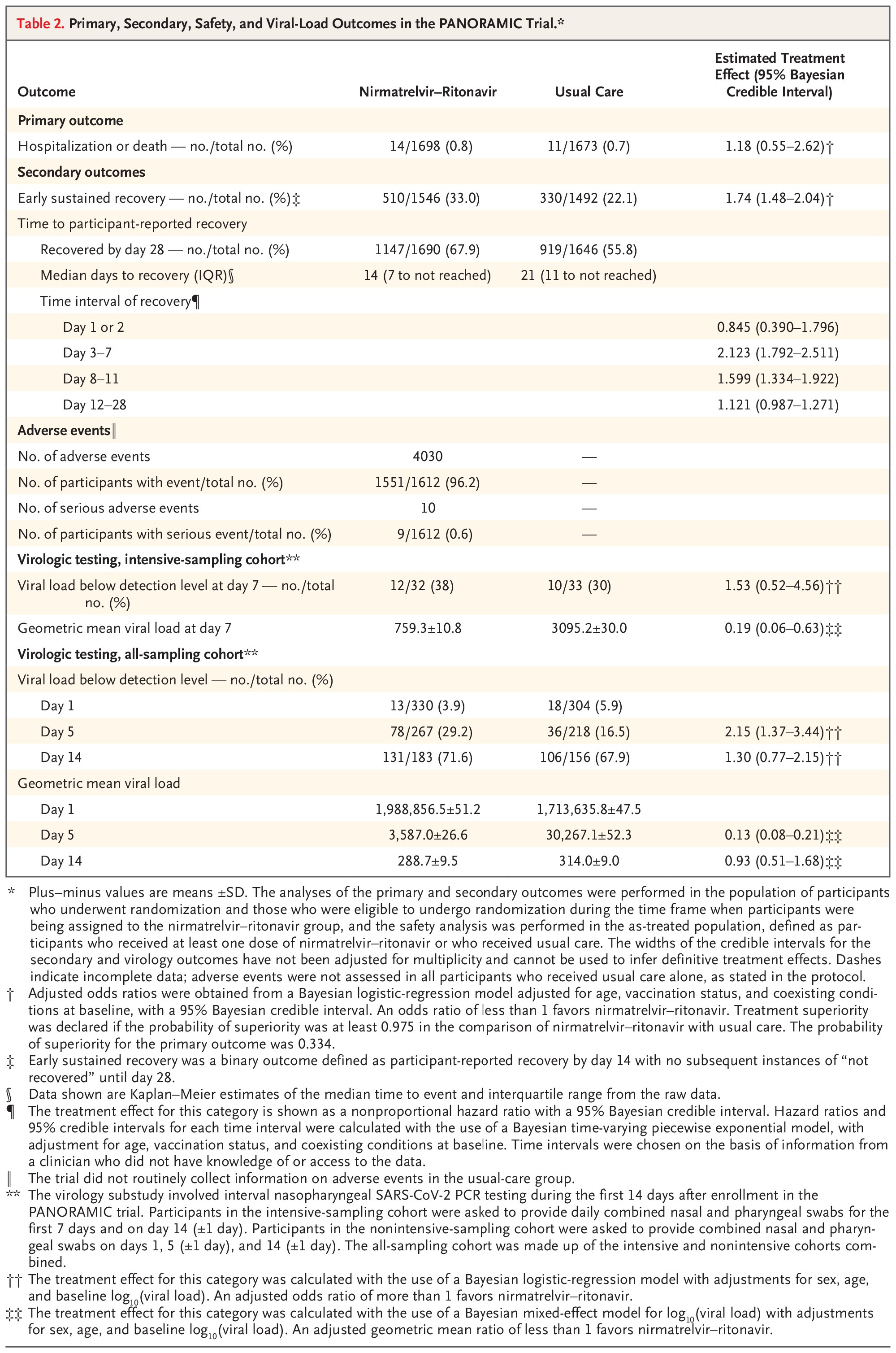
Table 2. Primary, Secondary, Safety, and Viral-Load Outcomes in the PANORAMIC Trial.<xref ref-type=”table-fn” rid=”t2fn1”>*</xref>
Oral Nirmatrelvir–Ritonavir for Covid-19 in Higher-Risk Outpatients. N Engl J Med. April 22, 2026.
Used under license from The New England Journal of Medicine.
Real-World Effectiveness Data
Multiple large observational studies and meta-analyses consistently demonstrate benefit, particularly in high-risk and older populations:
A meta-analysis of 30 cohort studies (462,279 nirmatrelvir-ritonavir recipients) found a 38% reduction in the composite of hospitalization or mortality (RR 0.62, 95% CI 0.55–0.70; moderate certainty), with no significant effect modification by vaccination status. [5]
A US Veterans Affairs target trial emulation (n=256,288) showed a relative risk of 0.60 (95% CI 0.50–0.71) in unvaccinated patients and 0.64 (0.58–0.71) in boosted patients, confirming benefit regardless of vaccination status. [6]
A large N3C cohort (n=703,647) estimated a 39% reduction in hospitalization and 61% reduction in death, with the greatest absolute benefit in patients aged ≥65 years. [7]
A Kaiser Permanente cohort study found 79.6% effectiveness when treatment was dispensed within 5 days of symptom onset, increasing to 89.6% when dispensed on the day of testing. [8]
A Québec population-based study (n=14,756 matched pairs) showed a 74% reduction in hospitalization (RR 0.26; NNT 15), with even greater benefit in incompletely vaccinated patients (RR 0.13; NNT 9) and immunocompromised individuals. [9]
IDSA Guideline Recommendations (2025)
The Infectious Diseases Society of America (IDSA) 2025 guideline synthesized RCT data showing an 83% relative risk reduction in hospitalization from two RCTs. For high-risk patients, this translates to an absolute reduction of 50 fewer hospitalizations per 1,000 (moderate certainty). For patients without risk factors, the absolute benefit is much smaller (~4 fewer per 1,000), limiting the usefulness of treatment in this population. Nirmatrelvir-ritonavir may also modestly accelerate symptom resolution in high-risk patients (HR 1.2, 95% CI 1.07–1.35). [10]
Summary
The totality of evidence supports nirmatrelvir-ritonavir as highly effective in reducing hospitalization and death in high-risk, unvaccinated patients (RRR ~89% in EPIC-HR). In vaccinated populations and during the Omicron era, the relative risk reduction remains significant (~35–74%), but the absolute benefit is smaller due to lower baseline event rates. The drug consistently accelerates symptom recovery and reduces viral load. Benefit is greatest when treatment is initiated early (within 5 days of symptom onset) and in patients aged ≥65 or with multiple comorbidities. For lower-risk or vaccinated patients without significant risk factors, the absolute benefit is modest.
Paxlovid. FDA Drug Label.
Food and Drug Administration. Updated date: 2026-02-19.
Based on the following primary sources:
Assessing Participants’ Experiences With the COVID-19 Symptom Diary in a Clinical Trial.
Journal of Patient-Reported Outcomes. 2025. Brown TM, Kanu C, Harrington M.
EBioMedicine. 2025. Baniecki ML, Guan S, Rai DK, et al.
Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19.
The New England Journal of Medicine. 2022. Hammond J, Leister-Tebbe H, Gardner A, et al.RCT
Nirmatrelvir for Vaccinated or Unvaccinated Adult Outpatients with Covid-19.
The New England Journal of Medicine. 2024. Hammond J, Fountaine RJ, Yunis C, et al.RCT
Oral Nirmatrelvir–Ritonavir for Covid-19 in Higher-Risk Outpatients.
The New England Journal of Medicine. 2026. Butler CC, Pinto AD, Harris V, et al.NewRCT
The Journal of Antimicrobial Chemotherapy. 2024. Mesfin YM, Blais JE, Kibret KT, et al.SR
BMJ. 2023. Xie Y, Bowe B, Al-Aly Z.RCT
PLoS Medicine. 2025. Bhatia A, Preiss AJ, Xiao X, et al.
The Lancet. Infectious Diseases. 2023. Lewnard JA, McLaughlin JM, Malden D, et al.Observational
Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2025. Kaboré JL, Laffont B, Diop M, et al.New
Infectious Diseases Society of America. 2025. Amy Hirsch Shumaker, Adarsh Bhimraj, Roger Bedimo, et alGuideline.
So who is “First10EM.com” and why do they think Paxlovid doesn’t work?
First10EM.com is a for-profit commercial enterprise owned by Dr. Justin Morganstern, a Canadian Family and ER physician who sells resuscitation plans, EBM deep dives and critical appraisals. A review of his website reveals mostly reasonable evidence reviews, except for his take on Paxlovid.
His negative review of Paxlovid draws from the same studies cited above yet he comes to a completely different conclusion. How can that be? Perhaps the answer is preconceived bias. As Dr. Morgantstern states on the First10EM.com website:
“I think we rushed the use of Paxlovid in the first place, and have never been convinced there was real benefit.”
“Pfizer ran away with their bags full of cash, and basically no one is prescribing Paxlovid anymore.”
It is crucial to note that Dr. Morganstern’s interpretation of the data stands in sharp contradistinction to that which is noted above in the NEJM Open Evidence review. Apparently running away with bags of cash is only bad when Pfizer does it?
