

According to an invited review in the New England Journal of Medicine, testosterone treatment in middle-aged and older men with hypogonadism has moderate benefits primarily in sexual function, with more modest effects on other outcomes, and must be weighed against emerging safety signals. [1]
Established Benefits
The landmark Testosterone Trials (TTrials), which enrolled 790 men with a mean age of 72 years and mean baseline testosterone of 234 ng/dL, demonstrated that one year of transdermal testosterone treatment: [1]
Sexual function: Increased sexual activity, sexual desire, and erectile function — the most consistently demonstrated benefit across trials [1]
Anemia: Corrected unexplained anemia of aging [1]
Bone density: Increased volumetric and areal bone mineral density and estimated bone strength in the spine and hip [1]
Mood/depression: Slight decreases in depressive symptoms and slight improvements in mood [1]
Walking ability: Small improvement in walking distance, though this was not significant in the primary Physical Function Trial analysis restricted to men with slow gait speed [1]
Notably, testosterone treatment did not improve vitality or cognitive function in the TTrials. [1]
Risks and Safety Considerations
The review highlights that testosterone treatment has been found to increase the risk of pulmonary embolism and clinical fractures, and it may increase the risk of atrial fibrillation. [1] However, testosterone treatment has not been shown to increase the risk of major adverse cardiovascular events (MACE), lower urinary tract symptoms, or prostate cancer in clinical trials. [1] The TRAVERSE trial, which was specifically designed to assess cardiovascular safety, confirmed no increase in MACE but did identify the increased fracture risk. [1]
Who Should Be Treated
Benefits can be expected only in men with unequivocal hypogonadism based on two or more measurements of fasting, early-morning testosterone levels below the lower limit of the normal range. [1] The lower the testosterone level (e.g., <200 ng/dL), the greater the likelihood of benefit. A benefit is less likely in men whose testosterone levels are only slightly below normal, especially those with obesity and metabolic disorders. [1] Testosterone consistently improves libido but may not be effective when the primary symptom is erectile dysfunction. [1]
Before initiating treatment, baseline evaluation for prostate cancer risk and lower urinary tract symptoms is recommended. Prophylactic anticoagulant therapy should be considered in men with a previous thromboembolic event, and men at high risk for fracture should be treated with osteoporosis medication. [1] The risk of erythrocytosis can be minimized by monitoring hematocrit and adjusting the testosterone dose to maintain physiologic levels. [1]
Testosterone Treatment in Middle-Aged and Older Men with Hypogonadism.
Bhasin S, Snyder PJ. The New England Journal of Medicine. 2025;393(6):581-591. doi:10.1056/NEJMra2404637.
Used under license from The New England Journal of Medicine.
Guideline Recommendations
Major society guidelines converge on an individualized approach. The Endocrine Society (2018) recommends against routine testosterone therapy in all older men with low testosterone but suggests consideration on an individualized basis in men with consistently low levels and symptoms suggestive of deficiency. [2-3] The American College of Physicians (2020) conditionally recommends discussing testosterone treatment specifically in men with age-related low testosterone and sexual dysfunction who want to improve sexual function, noting little to no evidence of benefit for physical function, depressive symptoms, energy, vitality, or cognition. [4] The European Male Ageing Study (EMAS) position statement (2023) similarly recommends TRT only for symptomatic older men with confirmed low testosterone, and specifically advises against routine use to improve exercise capacity, physical function, or cognitive function. [5]
The following table from a recent JAMA review summarizes the key outcomes from the TTrials substudies:
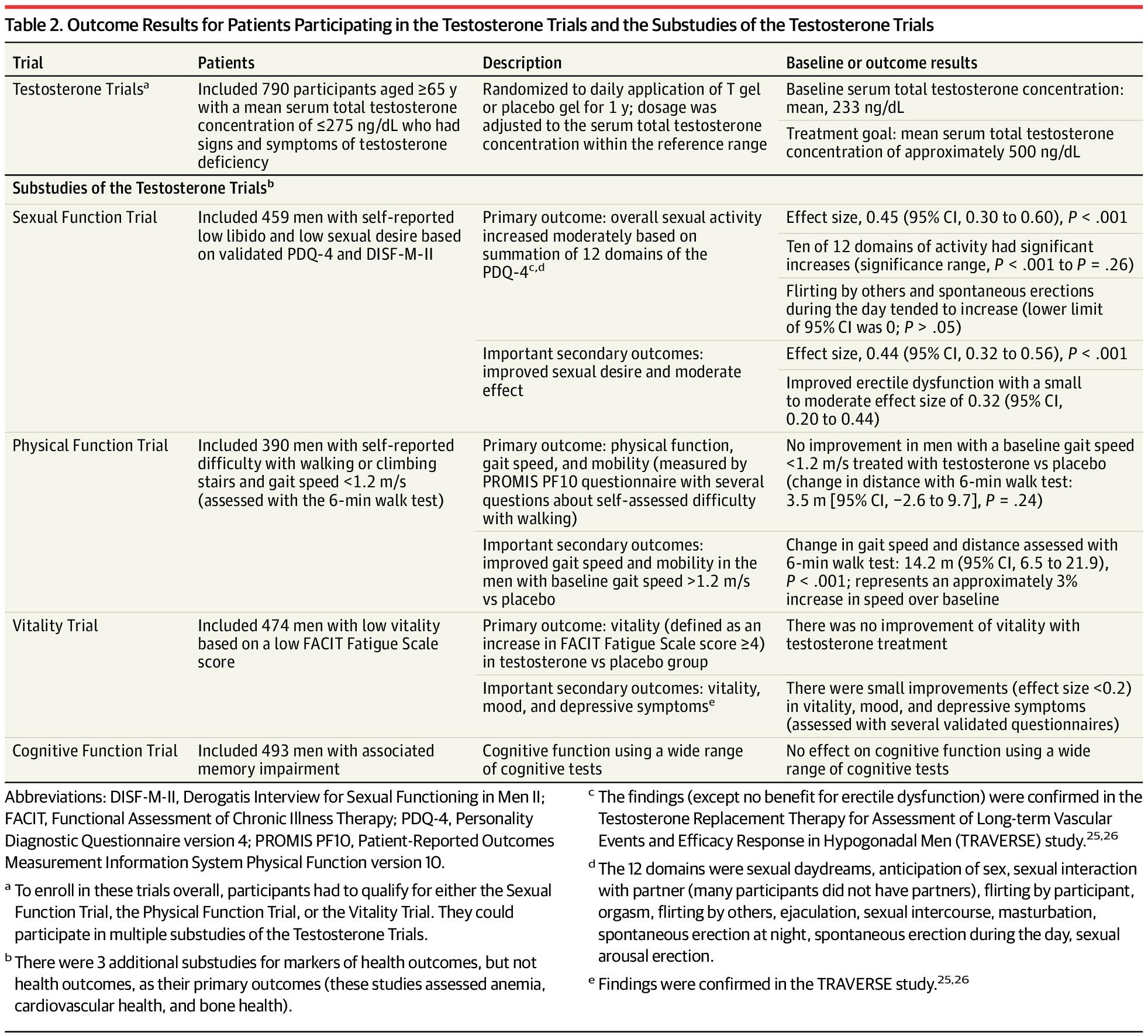
Table 2. Outcome Results for Patients Participating in the Testosterone Trials and the Substudies of the Testosterone Trials
Adult Male Hypogonadism. JAMA. May 27, 2026.
Content used under license from the JAMA Network®
© American Medical Association
Monitoring Requirements
Older men on testosterone should be monitored at 3, 6, and 12 months after initiation and at least yearly thereafter, with assessment of clinical response, total testosterone, hematocrit, and PSA concentrations. [5] Short-acting transdermal preparations are generally preferred for initiation in older men. [1][5]
Key Takeaway
The evidence supports that testosterone supplementation in men over 70 offers the most reliable benefit for sexual function and correction of anemia in those with confirmed hypogonadism, with smaller benefits for bone density and mood. However, the increased risk of pulmonary embolism and fractures, along with uncertainties about long-term safety, necessitate careful individualized risk-benefit assessment. [1][3][7]
Would you like to explore the specific findings from the TRAVERSE trial regarding cardiovascular and fracture outcomes in more detail?
1.
Testosterone Treatment in Middle-Aged and Older Men with Hypogonadism.
The New England Journal of Medicine. 2025. Bhasin S, Snyder PJ.RecentReview
2.
Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline.
The Journal of Clinical Endocrinology and Metabolism. 2018. Bhasin S, Brito JP, Cunningham GR, et al.Guideline
3.
Benefits and Risks of Testosterone Treatment in Men With Age-Related Decline in Testosterone.
Annual Review of Medicine. 2021. Rodrigues Dos Santos M, Bhasin S.Review
4.
Annals of Internal Medicine. 2020. Qaseem A, Horwitch CA, Vijan S, et al.Guideline
5.
EMAS Position Statement: Testosterone Replacement Therapy in Older Men.
Maturitas. 2023. Kanakis GA, Pofi R, Goulis DG, et al.
6.
The Journal of the American Medical Association. 2026. Anawalt BD, O’Connor KM, Grossmann M.RecentReview
7.
Benefits and Risks of Testosterone Treatment of Older Men With Hypogonadism.
The Urologic Clinics of North America. 2022. Galbiati FF, Goldman AL, Gattu A, Guzelce EC, Bhasin S.Review
The Schedule III designation creates practical regulatory burdens but has not been a major barrier to appropriate testosterone prescribing in the United States — in fact, testosterone use has tripled in recent years despite this classification. [1] The more significant barriers to treatment appear to be FDA labeling restrictions, prescriber hesitancy related to safety concerns, and insurance/reimbursement policies rather than the controlled substance scheduling itself.
Practical Implications of Schedule III Classification
As a Schedule III controlled substance under the Controlled Substances Act, all testosterone formulations carry specific regulatory requirements: [2-4]
Prescribers must hold a valid DEA registration
Prescriptions are limited to a maximum of 5 refills within 6 months of the original prescription date (unlike non-controlled medications, which allow up to 11 refills over 12 months)
Pharmacies must maintain controlled substance inventory records and report dispensing data to state prescription drug monitoring programs (PDMPs)
Some states impose additional restrictions on prescribing or dispensing
These requirements add administrative friction — particularly the need for more frequent office visits or prescription renewals — but have not prevented the dramatic expansion of testosterone prescribing observed over the past two decades. [1]
More Impactful Barriers
The literature suggests that other factors are more consequential barriers than the Schedule III designation:
FDA labeling restrictions: The FDA requires that testosterone products be labeled only for men with low testosterone due to known medical causes (primary or secondary hypogonadism), not for age-related decline alone. This creates a tension with clinical practice, where many prescriptions are written for men with age-related low testosterone. [1][5]
Prescriber hesitancy: FDA safety warnings, cardiovascular safety concerns, and diagnostic ambiguity around age-related hypogonadism have led some physicians to exercise caution in prescribing. Variation in prescribing across practices has been attributed to clinician beliefs about the appropriateness of TRT and diagnostic uncertainty. [6]
Reimbursement and insurance policies: In countries with stricter reimbursement criteria (e.g., Australia’s PBS system requiring specialist initiation), tightened prescribing rules have effectively curbed off-label use while preserving access for valid indications. In the U.S., prior authorization requirements from insurers can similarly delay or limit access. [7]
Cost considerations: The ACP specifically recommends considering intramuscular formulations over transdermal preparations when initiating treatment, as costs are considerably lower with similar clinical effectiveness. [5]
Paradox of the Schedule III Designation
Despite the controlled substance classification, testosterone prescribing in the U.S. has been characterized by substantial off-label use — with a significant proportion of men not even having testosterone levels tested before initiation of therapy. [1] This suggests the Schedule III designation has not functioned as a meaningful gatekeeper. The more effective regulatory lever has been the FDA’s 2015 labeling change restricting approved indications and requiring cardiovascular risk warnings, along with insurance prior authorization requirements. [7]
Would you like to explore the specific FDA labeling requirements and how they interact with prescribing for age-related hypogonadism versus classical hypogonadism?
1.
Annals of Internal Medicine. 2020. Diem SJ, Greer NL, MacDonald R, et al.Guideline
2.
Testosterone. FDA Drug Label.
Food and Drug Administration. Updated date: 2024-09-30.
3.
TESTOSTERONE ENANTHATE. FDA Drug Label.
Food and Drug Administration. Updated date: 2026-06-12.
4.
Testosterone Cypionate. FDA Drug Label.
Food and Drug Administration. Updated date: 2025-08-22.
5.
Annals of Internal Medicine. 2020. Qaseem A, Horwitch CA, Vijan S, et al.Guideline
6.
Clinical characteristics and comorbidities associated with testosterone prescribing in men.
Clinical Endocrinology. 2022. Sharma A, Ul-Haq Z, Sindi E, et al.
7.
Pharmacoepidemiology and Drug Safety. 2020. Handelsman DJ.
The Schedule III designation impacts primary care testosterone prescribing through several indirect mechanisms — administrative burden, PDMP requirements, and prescriber caution — though the controlled substance classification alone has not prevented primary care physicians from being the dominant prescribers of testosterone in the U.S. [1-3]
Primary Care Physicians Are the Leading Prescribers
Despite the Schedule III classification, family practice and internal medicine physicians collectively write more testosterone prescriptions than any specialty group. A 5-year CMS Medicare analysis (2013–2017) found that family practice and internal medicine were the top two specialties by prescription frequency, followed by urology and endocrinology. [2] Similarly, a Medicare prescriber analysis (2016–2019) confirmed this ordering, with the number of testosterone prescribers growing by a mean of 8.8% annually across specialties. [3] In the VA system, primary care providers were the most common prescribers, though endocrinologists and urologists were more likely to prescribe per provider and more likely to obtain appropriate pre-treatment workup. [4]
How Schedule III Requirements Affect Primary Care Workflow
The controlled substance designation creates several workflow-level frictions that disproportionately affect high-volume primary care settings:
PDMP consultation requirements: Most states now mandate or strongly recommend PDMP queries before prescribing any controlled substance (Schedules II–V). Physicians who frequently use PDMPs have over twice the odds of reducing or eliminating controlled substance prescriptions compared to those who never use them, suggesting the monitoring infrastructure itself has a chilling effect on prescribing. Low PDMP querying rates (as low as 52% even in mandate states) reflect clinician perceptions that the process is burdensome and time-consuming. [5-6]
Refill limitations: Schedule III prescriptions are limited to 5 refills within 6 months, requiring more frequent patient encounters or prescription renewals compared to non-controlled medications — a meaningful administrative burden in busy primary care practices. [7]
DEA registration and documentation: All prescribers must maintain active DEA registration and comply with controlled substance recordkeeping requirements, adding a layer of regulatory oversight that some clinicians find deterring. [8]
Telemedicine restrictions: DEA rules require that telemedicine prescribers of Schedule III medications provide only a 30-day initial supply before an in-person or surrogate evaluation is completed, limiting the growing role of telehealth in testosterone management. [9]
Prescriber Behavior and Variation
The key factors influencing primary care testosterone prescribing extend beyond scheduling alone. Diagnostic ambiguity around age-related hypogonadism, individual clinician beliefs about the appropriateness of TRT, and variation in local guidance all contribute to wide prescribing variation across practices. [10] A UK study found that variation in testosterone prescribing across over 6,700 general practices was largely attributable to unidentified factors such as GP choice and preference. [10] In the VA system, younger providers with less institutional experience were more likely to prescribe testosterone, while primary care providers were less likely than specialists to obtain guideline-concordant pre-treatment evaluation. [4]
Notably, a substantial proportion of men receiving testosterone in primary care do not have testosterone levels tested before initiation — approximately 25% in some estimates — and among those tested, roughly 20% had levels above 300 ng/dL, suggesting that the Schedule III designation has not functioned as an effective quality gatekeeper. [11-12]
Lessons from Stricter Regulatory Models
The Australian experience provides a natural experiment. When Australia’s Pharmaceutical Benefits Scheme (PBS) tightened reimbursement rules in 2015 to require specialist initiation for new testosterone prescriptions, GP-initiated prescriptions dropped to near-zero while specialist prescriptions remained stable — effectively eliminating off-label “Low T” prescribing without restricting access for pathological hypogonadism. [13] The following figure illustrates this differential impact by prescriber type:
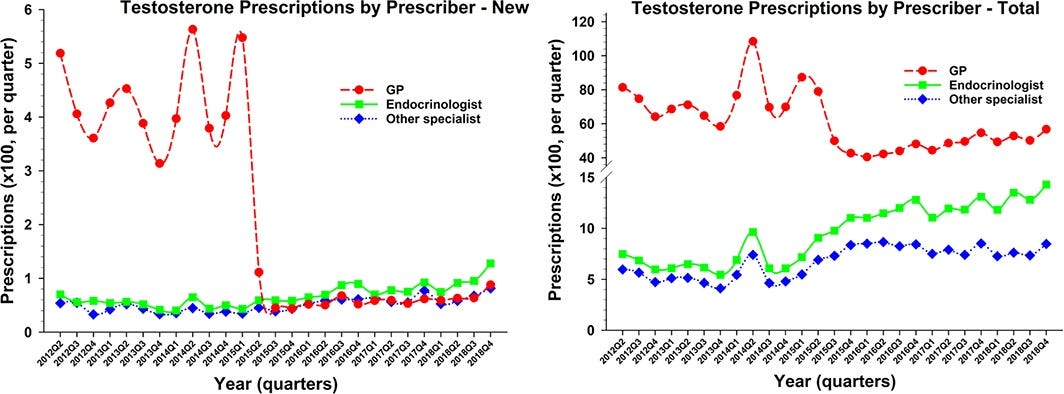
Figure 4. PBS testosterone prescription from 2012 to 2018 by quarter and by prescriber type consisting of GPs (red filled circles, dashed lines), endocrinologists (green filled squares, solid lines) and other specialists (blue filled stars, dotted lines).
Pharmacoepidemiology of testosterone: Impact of reimbursement policy on curbing off‐label prescribing. Pharmacoepidemiol Drug Saf. August 31, 2020.
This suggests that reimbursement and prescribing authority restrictions may be more effective levers than controlled substance scheduling for shaping appropriate prescribing patterns in primary care.
1.
Testosterone Therapy: Review of Clinical Applications.
American Family Physician. 2017. Petering RC, Brooks NA.Review
2.
Trends in Testosterone Prescription Amongst Medical Specialties: A 5-Year CMS Data Analysis.
International Journal of Impotence Research. 2023. Carter IV, Callegari MJ, Jella TK, et al.
3.
Trends in Testosterone Prescription During the Release of Society Guidelines.
International Journal of Impotence Research. 2024. Sellke N, Omil-Lima D, Sun HH, et al.
4.
Provider and Site-Level Determinants of Testosterone Prescribing in the Veterans Healthcare System.
The Journal of Clinical Endocrinology and Metabolism. 2017. Jasuja GK, Bhasin S, Rose AJ, et al.
5.
Journal of the American Medical Informatics Association : JAMIA. 2023. Mehta S, Brown W, Ferguson E, Najera J, Pantell MS.
6.
JAMA Health Forum. 2022. Neprash HT, Vock DM, Hanson A, et al.RCT
7.
Testosterone. FDA Drug Label.
Food and Drug Administration. Updated date: 2024-09-30.
8.
Policy and Medical-Legal Issues in the Prescribing of Controlled Substances.
Journal of Psychoactive Drugs. 1991. Clark HW.Review
9.
Rebalancing Controlled Substance Regulations in Telemedicine.
JAMA Health Forum. 2023. Kannarkat JT, Kannarkat JT, Torous J.Opinion
10.
Clinical characteristics and comorbidities associated with testosterone prescribing in men.
Clinical Endocrinology. 2022. Sharma A, Ul-Haq Z, Sindi E, et al.
11.
Annals of Internal Medicine. 2020. Diem SJ, Greer NL, MacDonald R, et al.Guideline
12.
Evaluation and Management of Testosterone Deficiency: AUA Guideline.
The Journal of Urology. 2018. Mulhall JP, Trost LW, Brannigan RE, et al.Guideline
13.
Pharmacoepidemiology and Drug Safety. 2020. Handelsman DJ.
Several distinct patient populations face disproportionate barriers to accessing testosterone therapy, driven by a combination of regulatory, socioeconomic, clinical, and systemic factors that interact differently across groups.
Transgender and Gender-Diverse Individuals
This population faces among the most significant access barriers. The Schedule III classification compounds existing challenges unique to this group:
Insurance denials and prior authorization: Over half (55%) of transgender individuals surveyed reported being denied coverage for transition-related surgery, and 25% were denied coverage for hormone therapy, despite evidence that such interventions are safe, effective, and medically necessary. Transmasculine individuals face gender-specific barriers resulting from regulations on masculinizing hormones, including restrictive formulary lists and letter requirements. [1-2]
Provider scarcity and stigma: A lack of providers trained or willing to prescribe gender-affirming hormone therapy (GAHT) is a major structural barrier. Nearly one-quarter of transgender respondents did not see a doctor when needed due to fear of mistreatment, and one-third reported negative healthcare experiences related to being transgender. Within the VA system, barriers include anticipated or enacted stigma and patient dissatisfaction with prescribing practices. [1][3]
Consequences of restricted access: Delays in accessing testosterone therapy for transgender individuals have been associated with worsened gender dysphoria, depression, and suicidality. A randomized trial demonstrated that earlier access to testosterone significantly reduced gender dysphoria and depression scores compared to delayed access. Individuals unable to access care through conventional channels may obtain hormones from unlicensed sources, risking inappropriate dosing. [1][4]
Racial and Ethnic Minorities
Non-white ethnicity and socioeconomic deprivation were independently associated with lower testosterone prescribing rates across over 6,700 general practices in England, even after adjusting for comorbidities and practice characteristics. In the U.S., testosterone therapy users are predominantly white, non-Hispanic, and located in the South and West Census regions. [5-6]
Paradoxically, the Endocrine Society guidelines recommend a lower PSA threshold (>3 ng/mL vs. >4 ng/mL) for urological evaluation before initiating testosterone in African American men and men with a first-degree relative with prostate cancer, creating an additional clinical gatekeeping step for this population. [7]
Socioeconomically Disadvantaged Populations
In Sweden, testosterone use was more common among men with higher household income — a pattern opposite to the prevalence of hypogonadism, suggesting socially conditioned under-prescribing in lower-income men with genuine deficiency. This disparity persisted despite pharmaceutical benefits coverage, suggesting that health-seeking behavior and prescribing practices, rather than affordability alone, drive the gap. [8]
Cost differentials between formulations create access tiers: intramuscular testosterone costs approximately $156/year vs. $2,135/year for transdermal formulations. Direct-to-consumer telemedicine platforms charge $1,586–$4,200 annually, far exceeding costs at tertiary centers with insurance coverage. Patients without insurance or with high-deductible plans face substantially greater out-of-pocket burden. [9-10]
Insurance transparency is poor — only 62% of major U.S. health plans had publicly accessible policies regarding hypogonadism coverage, compared to 94% for breast reconstruction. [11]
Men with HIV
Hypogonadism prevalence among men living with HIV remains 13–40% in the 20–60 age group, higher than age-matched HIV-uninfected men. [12] Despite Endocrine Society recommendations for testosterone therapy in symptomatic HIV-associated hypogonadism, this population faces unique barriers:
Uncertainty about whether hypogonadism diagnosed at the time of HIV diagnosis persists after immune recovery on antiretroviral therapy, leading to prescriber hesitancy. [13]
The functional (rather than organic) nature of hypogonadism in many men with HIV complicates the decision to initiate therapy. [12]
Following FDA cardiovascular safety warnings, testosterone use declined in the general population but less so among men with HIV, suggesting this population may be more dependent on continued therapy. [13]
Opioid-Induced Hypogonadism
Men on chronic opioid therapy represent a large and growing population with secondary hypogonadism. Opioids suppress the hypothalamic-pituitary-gonadal axis, and the Endocrine Society identifies opioid use as a condition warranting testosterone measurement. [7] However, these patients face compounded controlled substance barriers — both their opioid and their testosterone require Schedule II/III prescriptions, PDMP monitoring, and frequent follow-up, creating substantial administrative burden for both patients and prescribers.
Older Men (>70 years)
Despite having the highest prevalence of low testosterone (approximately 30% in men >70 and 50% in men >80), older men show decreasing testosterone use with increasing age — the inverse of the epidemiologic need. [8-9] Contributing factors include more comorbidities that serve as relative contraindications (cardiovascular disease, polycythemia), prescriber reluctance due to safety concerns, and the FDA’s restriction of approved indications to pathological hypogonadism rather than age-related decline. [9]
1.
Health Care for Transgender and Gender Diverse Individuals: ACOG Committee Opinion, Number 823.
Obstetrics and Gynecology. 2021. Committee on Gynecologic Practice and Committee on Health Care for Underserved WomenGuideline
2.
Social Science & Medicine. 2025. D’Angelo AB, Dearolf M, Restar A, et al.
3.
Barriers and Facilitators to Gender-Affirming Hormone Therapy in the Veterans Health Administration.
Annals of Behavioral Medicine : A Publication of the Society of Behavioral Medicine. 2023. Wolfe HL, Boyer TL, Shipherd JC, et al.
4.
JAMA Network Open. 2023. Nolan BJ, Zwickl S, Locke P, Zajac JD, Cheung AS.RCT
5.
Clinical Endocrinology. 2021. Heald AH, Stedman M, Whyte M, et al.
6.
Trends and Patterns of Testosterone Therapy Among U.S. Male Medicare Beneficiaries, 1999 to 2014.
The Journal of Urology. 2020. Zhou CK, Advani S, Chaloux M, et al.
7.
Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline.
The Journal of Clinical Endocrinology and Metabolism. 2018. Bhasin S, Brito JP, Cunningham GR, et al.Guideline
8.
Testosterone prescribing in the population—a short social epidemiological analysis in Sweden.
Pharmacoepidemiology and Drug Safety. 2016. Bjerkeli PJ, Mulinari S, Merlo J.
9.
Annals of Internal Medicine. 2020. Qaseem A, Horwitch CA, Vijan S, et al.Guideline
10.
The Journal of Sexual Medicine. 2022. Jesse E, Sellke N, Rivero MJ, et al.Observational
11.
Urology. 2017. Le B, McAchran S, Paolone D, et al.
12.
Update on Acquired Hypogonadism in Men Living With HIV: Pathogenesis, Clinic, and Treatment.
Frontiers in Endocrinology. 2023. De Vincentis S, Rochira V.Review
13.
Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024. Horberg M, Thompson M, Agwu A, et al.Guideline
NEJM Review
According to an invited review in the New England Journal of Medicine, a subset of older men with unequivocal hypogonadism may benefit from testosterone therapy, but the decision requires careful individualized balancing of benefits against emerging safety signals. [1]
The review identifies several domains where testosterone treatment has demonstrated benefit in middle-aged and older men with hypogonadism: improved libido, sexual activity, and erectile function; correction of anemia; and slight improvements in depressive symptoms, mood, energy, and walking ability. [1] However, the magnitude of benefit is closely tied to the degree of testosterone deficiency — the lower the testosterone level (e.g., <200 ng/dL), the greater the likelihood of benefit. Men whose levels are only slightly below the lower limit of normal, particularly those with obesity and metabolic disorders, are less likely to benefit. [1]
Critically, the review highlights that the risk profile has evolved with new data. While the TRAVERSE trial established that testosterone treatment does not increase the risk of major adverse cardiovascular events (MACE), it revealed that testosterone increases the risk of pulmonary embolism and, unexpectedly, clinical fractures — the latter a 43% increase, predominantly involving ankle, wrist, and rib fractures. [1] The fracture finding was particularly surprising given that testosterone consistently improves bone mineral density and architecture; the review speculates that increased physical activity may have contributed, though this was not assessed. [1] Testosterone may also increase the risk of atrial fibrillation. [1]
The review recommends that if testosterone treatment is considered warranted based on expected benefit, the expected risk should be minimized through baseline evaluation for prostate cancer risk and lower urinary tract symptoms, and prophylactic anticoagulant therapy should be considered in men with a history of thromboembolic events. [1] Testosterone consistently improves libido but may not be effective when the primary symptom is erectile dysfunction alone. [1]
Testosterone Treatment in Middle-Aged and Older Men with Hypogonadism.
Bhasin S, Snyder PJ. The New England Journal of Medicine. 2025;393(6):581-591. doi:10.1056/NEJMra2404637.
Used under license from The New England Journal of Medicine.
The Gap Between Prevalence and Treatment
There is a substantial population of older men who are potentially undertreated. The prevalence of low testosterone is approximately 20% in men over 60, 30% in men over 70, and 50% in men over 80. [2] However, the prevalence of syndromic late-onset hypogonadism — defined as at least three sexual symptoms with confirmed low testosterone — is considerably lower, estimated at 3.2% of men aged 60–69 and 5.1% of men aged 70–79 in the European Male Ageing Study. [3] This distinction is clinically important: many men with biochemically low testosterone are asymptomatic or have symptoms attributable to comorbidities rather than androgen deficiency.
What the Evidence Supports
The strongest evidence for benefit in older men comes from the TTrials (men ≥65 with testosterone <275 ng/dL) and the TRAVERSE trial, which together demonstrate: [4-6]
Sexual function: Moderate improvements in sexual activity, desire, and erectile function — the most consistent and clinically meaningful benefit
Anemia: Correction of unexplained anemia of aging, with a greater proportion achieving hemoglobin increments >1 g/dL
Bone density: Increased volumetric and areal BMD at spine and hip — though the TRAVERSE fracture substudy paradoxically showed a 43% increase in clinical fractures, raising questions about whether BMD improvement translates to fracture reduction in this population [1][7]
Mood: Small improvements in depressive symptoms
Physical function: Modest improvements in walking distance, though not in the primary physical function endpoint of the TTrials
The following figure from the TRAVERSE fracture substudy illustrates the unexpected finding of increased fracture risk across all fracture types:
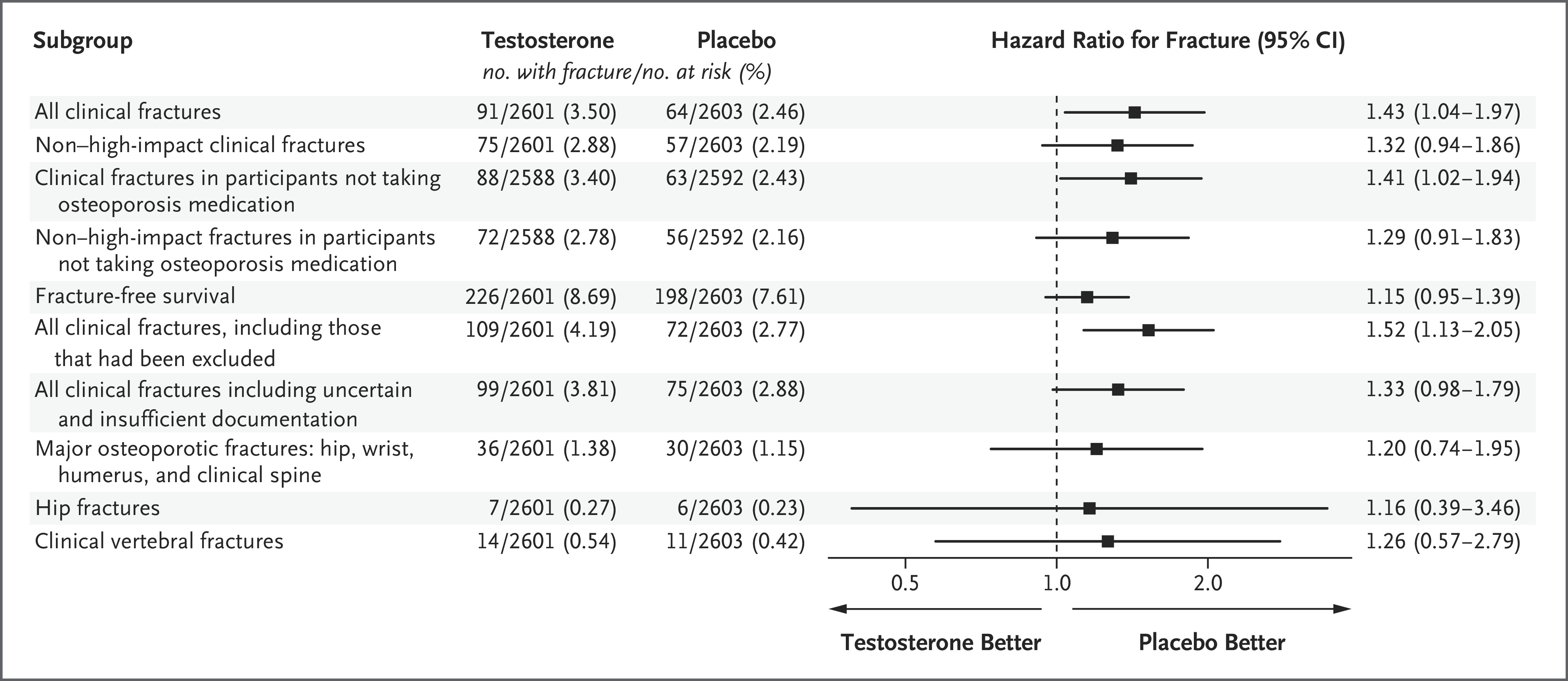
Figure 1. Fracture End Points.
Testosterone Treatment and Fractures in Men with Hypogonadism. N Engl J Med. January 17, 2024.
Used under license from The New England Journal of Medicine.
Cardiovascular Safety Is Now Better Defined
The TRAVERSE trial (n=5,246; mean follow-up 33 months) demonstrated noninferiority of testosterone to placebo for MACE (HR 0.96; 95% CI 0.78–1.17), effectively resolving a decade of uncertainty. [6] However, non-MACE signals warrant monitoring: numerically higher rates of atrial fibrillation (3.1% vs. 2.4%), pulmonary embolism (0.9% vs. 0.5%), and acute kidney injury (2.3% vs. 1.5%) were observed in the testosterone arm, and erythrocytosis was the most reproducible adverse effect (17.0% vs. 3.3%). [9]
Guideline Consensus and the Case for Individualization
All major guidelines converge on the same framework: not routine treatment for all older men, but individualized therapy for selected symptomatic men with confirmed low testosterone. [2][4][10]
The Endocrine Society recommends against routinely prescribing testosterone to all men ≥65 with low levels, but suggests individualized treatment for those with symptoms such as low libido or unexplained anemia and consistently low morning testosterone. [4]
The ACP limits its conditional recommendation to men with age-related low testosterone and sexual dysfunction, recommending discontinuation if no improvement occurs within 12 months. [2]
The EMAS (2023) adds that testosterone may be considered for hypogonadal men with severe insulin resistance/pre-diabetes, osteoporosis (in combination with proven treatments), or persistent mild depressive symptoms. [10]
An important consideration is that functional hypogonadism — driven by obesity, metabolic syndrome, or medications — may respond to addressing the underlying cause rather than testosterone supplementation. Weight loss through lifestyle intervention or GLP-1/GIP agonists has been shown to normalize testosterone in up to 81–89% of men at 6–24 months after bariatric surgery. [9]
In summary, more older men likely could benefit from testosterone therapy than currently receive it, particularly those with unequivocally low testosterone (<200 ng/dL), sexual symptoms, or unexplained anemia. However, the emerging fracture signal, thromboembolic risk, and the importance of distinguishing organic from functional hypogonadism argue against broadening treatment indiscriminately. The greatest opportunity may lie in better identification and evaluation of symptomatic older men rather than lowering the threshold for treatment.
